 Osteoblasts are the cells involved
in bone deposition, the formation of new bone. They are
connective tissue cells found at the surface of bone. They can be
stimulated to proliferate and differentiate into osteocytes.
Osteoblasts are the cells involved
in bone deposition, the formation of new bone. They are
connective tissue cells found at the surface of bone. They can be
stimulated to proliferate and differentiate into osteocytes.Bone may seem to be stable and unchanging, but in fact, bone is
constantly being remodeled. Bone remodeling can be broken down
into two processes: bone
resorption and bone
deposition. In bone resorption, the collagen
and other proteins in bone tissue are digested by proteases, and
bone mineral is dissolved to release calcium and phosphate to the
extracellular fluid. Bone deposition is the process whereby
new bone is formed.
To understand bone remodeling, and the factors that lead to pathological problems with bone, you need to know about three cell types found in bone.
Osteoblasts are the cells involved
in bone deposition, the formation of new bone. They are
connective tissue cells found at the surface of bone. They can be
stimulated to proliferate and differentiate into osteocytes.
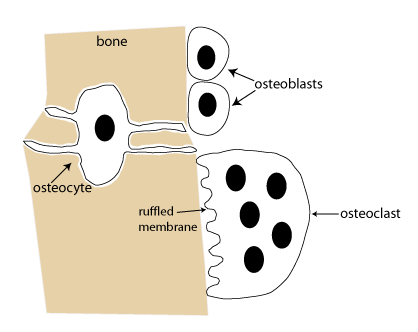
Osteocytes are bone cells. Osteocytes manufacture collagen and other substances that make up the bone extracellular matrix. Osteocytes are enclosed in bone.
Osteoclasts are bone-resorbing cells ("-clast" means to break; osteoclasts break down bone). They are large, multinucleate cells that form through the fusion of precursor cells. Unlike osteoblasts, which are related to fibroblasts and other connective tissue cells, osteoclasts are related to white blood cells that are phagocytes. "-Phage" means to eat, and phagocytes are specialized to engulf and digest pathogens and other cellular debris.
Certain signals are required to cause precursor cells to fuse and
generate osteoclasts (see below). After osteoclasts form,
the first step necessary for bone resorption to occur is that the
mature osteoclast needs to tightly adhere to the bone, creating a
specialized compartment that is isolated from surrounding tissue.
Once the osteoclast adheres to the bone surface, the membrane
adjacent to the bone differentiates as the ruffled membrane.
The ruffled membrane contains proteins that pump acid into the
isolated compartment next to the bone. The acid dissolves the
minerals in the bone; subsequently, proteases are secreted into
the compartment. Proteases are enzymes that break down
collagen and other proteins. Bone resorption ends when the
osteoclast dies by apoptosis.
The process of bone remodelling begins when bone resorption is triggered by various signals. One signal is the hormone parathyroid hormone (PTH), which gets released in response to a fall in the level of calcium in the extracellular fluid. PTH binds to receptors on osteoblasts and causes them to express a signal that stimulates the formation of osteoclasts. When osteoclasts form and cause some bone resorption, this releases calcium to the extracellular fluid to bring the level back to normal.
Another signal that can trigger bone remodeling is mechanical stress on bone. This is why weight-bearing exercise helps to strengthen bone tissue.
Importantly, signals that trigger bone resorption also stimulate
subsequent bone deposition through signals that promote the
proliferation and activity of osteoblasts. Normally, the level of
bone resorption and bone deposition is balanced, so that there is
no net loss of bone mass.
Osteoporosis is a severe reduction in bone mass that substantially increases the risk of bone fracture. Osteoporosis is diagnosed by measuring bone density (bone mass per unit volume) at different sites around the body.
The word "osteoporosis" means "holes in bone". In osteoporosis, bone resorption greatly outpaces bone deposition, causing a reduction of bone density and deterioration of bone architecture such that bones are fragile and susceptible to fracture. Osteoporosis is mainly seen in older women due to decreased estrogen levels following menopause. Estrogen helps maintain bone by inhibiting the development and activity of osteoclasts.
Everyone experiences bone loss as they age, but not everyone develops osteoporosis. A critical factor that will affect bone health as one ages is peak bone mass. The skeleton reaches full size at the end of puberty, but bone mass continues to increase and peak bone mass is attained in the mid-30's. Someone with a low peak bone mass is more likely to develop osteoporosis later in life. The development of a high peak bone mass will be a function of genetics, but is also influenced by good nutrition and exercise. Prevention of osteoporosis is focused on ensuring adequate dietary levels of calcium along with a healthy exercise regimen during the bone building years.
The goal of treatment for osteoporosis is to reduce the risk of
fracture. One way to do this is with an antiresorptive
therapy: in other words, one that
inhibits bone resorption. The first line treatment for
osteoporosis is with antiresorptive drugs called bisphosphonates.
Bisphosphonates can avidly bind to minerals in bone and inhibit
the activity of osteoclasts. Antiresorptive treatments are
able to reduce bone loss, but they do not work to build new bone.
This is one reason why preventive measures such as good nutrition
and exercise are so important.
Another way to build bone density is with an anabolic therapy,
which is capable of stimulating bone deposition. The main
anabolic therapies are drugs that mimic the hormone PTH.
Despite the role of PTH in stimulating bone resorption, it turns
out that if given as a once-daily injection, PTH agonists
stimulate osteoblasts to promote bone
deposition.
The newest anabolic treatment for osteoporosis (approved in April 2019) is romosozumab, a monoclonal antibody drug that inhibits the signaling molecule sclerostin. Sclerostin signaling normally acts to limit bone deposition. Romosozumab must be administered by injection and is only recommended for women with severe osteoporosis who have failed other treatments.
Through the early 2000s, the mainstay of osteoporosis treatment in post-menopausal women was hormone replacement therapy (HRT) with estrogen and progesterone. The Women's Health Initiative was a large study that showed that HRT can reduce the risk of fractures. However, this study also showed that HRT causes a greater risk of adverse cardiovascular events, as well as an increased risk of breast cancer. For this reason, there has been a large drop in prescriptions for HRT, and it is no longer recommended for the treatment of osteoporosis.