Brain Anatomy: Clinical Examples
Visual Pathways into the CNS
In the visual system, the retina at the back of the
eyeball contains the photoreceptors that detect light, along with
other types of cells that process the visual signal. The output
from the retina to the brain is from the retinal ganglion
cells, whose axons project to the thalamus
via the optic nerve, optic chiasm, and optic tract.
Refer to figure 10.34 on p. 350 of the textbook. The retina can
be divided into two halves: the nasal retina, which is
closer to the nose, and the temporal retina, which is closer to
the temporal bone and in a lateral position. See which
retinal ganglion cells encode information about the right visual
field (indicated by the red lines in the schematic drawing).
Essentially, the right visual field is "looked at" by the left
temporal retina and the right nasal retina. The projection into
the brain is organized so that all of the information about the
right visual field will end up in the left thalamus and left
visual cortex. This is achieved because the axons from ganglion
cells in the nasal retina cross over at the optic chiasm, while
axons from the temporal retina do not cross to the other side.
The clinical significance of this anatomical arrangement is that
certain disorders may cause partial visual field losses known as hemianopias (also called
hemianopsias). The pituitary gland sits just behind and
below the optic chiasm. Sometimes tumors in the pituitary gland
will specifically compress axons in the center of the optic
chiasm. This causes a loss of peripheral vision
(specifically the term is bitemporal hemianopia).
What happens if there is a lesion in the left optic tract?
answer
Be able to draw a schematic of the path taken by the axons from
the nasal and temporal halves of the retina, and know the effects
of lesions affecting the optic nerve, optic chiasm, and optic
tract.
Upper Motor Neuron Disorders
The primary motor cortex is
located in the precentral gyrus.
This region of the brain contains neurons that are involved in
initiating voluntary movements. A key feature about this region
(and the adjacent primary somatosensory cortex in the postcentral
gyrus) is that neurons are organized somatotopically.
This means that neurons that control muscles in adjacent parts of
the body are next to each other in the primary motor cortex.
Essentially, there is a map of the body in the brain. As
shown in figure 13.10 on p.427, regions of the body with more fine
motor control (such as the hand) have a higher degree of
representation in the motor cortex.
The neurons whose cell bodies are located in the primary motor
cortex are some of the largest neurons in the body. The axons of
these neurons extend down to the spinal cord where they make
direct synaptic connections with somatic motor neurons (cells that
innervate skeletal muscles). A clinical term for these cells in
the motor cortex is upper motor neurons
(with the somatic motor neurons being the lower motor neurons).
Another name for these cells is pyramidal neurons, because
their axons cross in a structure on the ventral surface of the
medulla known as the pyramids.
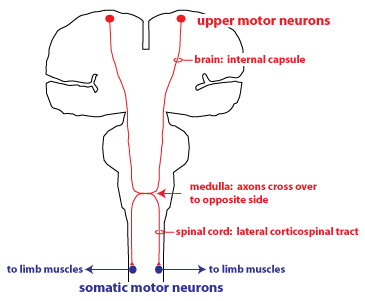 The
axon bundle containing the axons of the upper motor neurons is
termed the corticospinal tract.
Axons in the first part of the corticospinal tract are found in a
region of white matter called the internal
capsule. The internal capsule can best be seen in
the horizontal
section of the brain, dividing different nuclei in the basal
ganglia (but is also visible in one of the frontal sections). Most
of the axons (particularly those that project to somatic motor
neurons innervating the limbs) cross over to the opposite side of
the body at the medulla oblongata,
and then continue in the spinal cord in the lateral corticospinal
tract. This is schematized in the figure at right.
The
axon bundle containing the axons of the upper motor neurons is
termed the corticospinal tract.
Axons in the first part of the corticospinal tract are found in a
region of white matter called the internal
capsule. The internal capsule can best be seen in
the horizontal
section of the brain, dividing different nuclei in the basal
ganglia (but is also visible in one of the frontal sections). Most
of the axons (particularly those that project to somatic motor
neurons innervating the limbs) cross over to the opposite side of
the body at the medulla oblongata,
and then continue in the spinal cord in the lateral corticospinal
tract. This is schematized in the figure at right.
Damage to neurons of the corticospinal tract is known clinically
as an upper motor neuron disorder.
An upper motor neuron disorder will affect motor control in
different ways, depending on the location of the damage. If a
stroke causes a lesion in the primary motor cortex, motor function
on the opposite (contralateral) side of the body will be affected.
If on the other hand, there is damage to the lateral spinal cord
where the lateral corticospinal tracts are located, this will
cause a motor defect in the limbs on the same
(ipsilateral) side of the body.
Damage to the upper motor neurons causes two kinds of effects.
The predominant effect initially is a loss of motor function,
either paralysis or muscle weakness. These changes
result from loss of excitatory input to the somatic motor neurons,
and are termed a negative signs. However some of the axons
that descend in the corticospinal tract provide inhibitory
input to neurons in the spinal cord, and loss of this input
leads to abnormal increases in certain motor behaviors, or positive
signs. An example of a positive sign is exaggerated
reflexes (hyperreflexia). Another positive
sign is an increase in stiffness, or muscle tone (hypertonia).
Muscle tone is defined as the resistance of the muscle to passive
stretch.
Parkinson's Disease
Parkinson's disease is a neurodegenerative disease affecting the
basal ganglia, which are involved in the control of
movement. The disease is diagnosed by observing a set of
characteristic symptoms: resting tremor, bradykinesia, and
hypertonia.
- Resting tremor is an
oscillating movement that occurs when the patient is trying to
be still. The tremor usually disappears when the patient
undertakes a voluntary movement with the limb. This
distinguishes it from other disorders involving tremor in which
the tremor persists during movement (essential tremor) or is
specifically associated with movement (intention tremor in
cerebellar disorders).
- Bradykinesia means
slowness of movement. The patient might initially experience
bradykinesia as a weakness or stiffness in one limb.
- Hypertonia (excessive muscle tone) also occurs in
Parkinson's disease. This will manifest itself as rigidity or
stiffness.
Other typical features seen as the disease progresses are a
stooped posture and slow, shuffling gait. As it becomes more and
more difficult to initiate movement, the patient will start to
show akinesia, or a lack of movement. Lack of
movement of the facial muscles gives the patient the appearance of
having a mask-like, frozen look.
For many patients, the initial presentation is asymmetric,
meaning only one limb or one side of the body is affected. This is
what is illustrated in the video clip, from a clinical practice article
in the New England Journal of Medicine (Nutt JG and Wooten GF.
Diagnosis and Initial Management of Parkinson's Disease. N
Engl J Med 2005;353(10):1021-7).
The second video clip shows a patient in whom the
disease is much more advanced. The patient has a strong resting
tremor in the arms, and a stooped posture. Akinesia manifests as
"freezing of gait", in which the patient has great difficulty in
taking a step forward. Amazingly, the second part of the video
shows the patient is still able to ride a bicycle. (Snijders, A.
H. and Bloem, B. R. Cycling for Freezing of Gait. N Engl J Med
2010;362: e46).
Neurodegeneration in Parkinson's Disease
 Parkinson’s disease is
caused by a degeneration of neurons in the substantia
nigra of the midbrain. Substantia nigra means
"black substance, and it is easily reconizable as the pigmented
region that stretches across the midbrain in a frontal section
of the brain. These neurons form connections with the basal ganglia and release the
neurotransmitter dopamine.
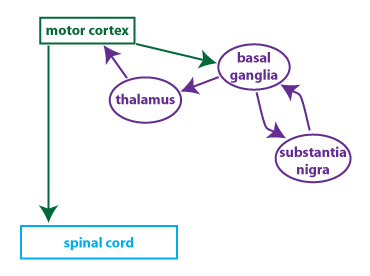
Parkinson's disease is considered a disorder of the basal ganglia
because the major projection from the substantia nigra is to
nuclei of the basal ganglia*. The schematic provides a simplified
illustration of the connectivity of the basal ganglia. The
basal ganglia receive inputs from the motor cortex (and other
brain regions), and then project back to the motor cortex via the
thalamus. The substantia nigra is interconnected with nuclei in
the basal ganglia. The basal ganglia integrate these
multiple inputs to modulate the output of the motor cortex. Some
of the connections are excitatory and some are inhibitory. The
loss of input from dopamine-releasing neurons in the substantia
nigra alters the balance of the output from the basal ganglia to
the motor cortex, and this underlies the symptoms that are seen.
Parkinson’s disease is
caused by a degeneration of neurons in the substantia
nigra of the midbrain. Substantia nigra means
"black substance, and it is easily reconizable as the pigmented
region that stretches across the midbrain in a frontal section
of the brain. These neurons form connections with the basal ganglia and release the
neurotransmitter dopamine.
Parkinson's disease is considered a disorder of the basal ganglia
because the major projection from the substantia nigra is to
nuclei of the basal ganglia*. The schematic provides a simplified
illustration of the connectivity of the basal ganglia. The
basal ganglia receive inputs from the motor cortex (and other
brain regions), and then project back to the motor cortex via the
thalamus. The substantia nigra is interconnected with nuclei in
the basal ganglia. The basal ganglia integrate these
multiple inputs to modulate the output of the motor cortex. Some
of the connections are excitatory and some are inhibitory. The
loss of input from dopamine-releasing neurons in the substantia
nigra alters the balance of the output from the basal ganglia to
the motor cortex, and this underlies the symptoms that are seen.
Parkinson's disease can be treated by restoring the dopamine that
is lost from the basal ganglia when neurons from the substantia
nigra degenerate. Dopamine itself cannot be used because it
doesn't cross the blood-brain barrier.
Instead, patients are treated with L-DOPA (also known as
levodopa), a dopamine precursor that can cross the blood-brain
barrier.
Optional
This video
shows the effectiveness of a treatment for Parkinson's disease
called deep brain stimulation (DBS). DBS changes the
activity of neurons in the basal ganglia circuitry in ways that
are not fully understood. The treatment doesn't work for all
Parkinson's patients, but for some individuals, DBS can have a
profound effect on symptoms.
*Wikipedia (and perhaps some other sources)
define the basal ganglia as "subcortical nuclei", a definition
that allows the substantia nigra to be lumped in with the
cerebral nuclei of the basal ganglia. For our purposes,
the basal ganglia consist of the three nuclei (caudate, putamen,
globus pallidus--you don't need to know the specific names)
located deep in the cerebrum. Functionally speaking, the
substantia nigra is part of the basal ganglia circuitry; but
anatomically speaking, it is a distinct nucleus located in the
midbrain.