Renal phosphate loss
Microscopic images
X-rays
Therapy
Phosphate supplements
Burosumab
Hypophosphatasia
Other notes
References
|
| Causes
Renal phosphate loss Microscopic images X-rays Therapy Phosphate supplements Burosumab Hypophosphatasia Other notes References |
Osteomalacia means "soft bones". Osteoid is the bone protein matrix, composed primarily of type 1 collagen. When there is insufficient mineral or osteoblast dysfunction, the osteoid does not mineralize properly, and it accumulates. The unmineralized osteoid has consistency similar to the tip of the nose, instead of the normal hard bone in the bridge of the nose.
Rickets is a problem near the joints when the bone formed by a growth plate does not mineralize. Then the growth plate becomes thick, wide and irregular. This is seen only in children because adults no longer have growth plates. However, the abnormal joints persist and adults can have deformities such as bowed legs. Most of the hereditary causes of osteomalacia appear during childhood and cause rickets.
Osteomalacia is uncommon. Patients are often short. They have bowed legs and may have large skulls and prominent foreheads. Lumps occur where the ribs join the sternum ("the rachetic rosary). The bones may be painful. The diagnosis is often made in young children because they don't walk, due to painful knees. Frequently patients have problems with development of teeth.
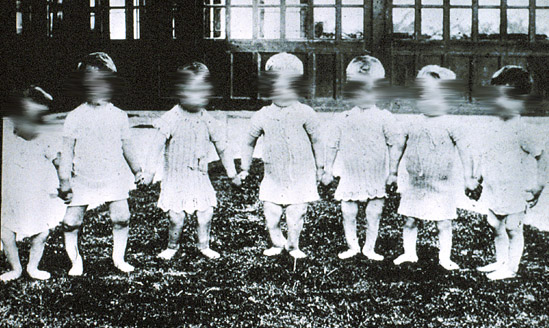
When children do not get enough vitamin D in their diet and also don't get adequate sunlight exposure to their skin, they develop rickets. This photograph was taken over 100 years ago in a Scottish orphanage, before the importance of vitamin D was recognized.
The following table lists the causes of osteomalacia and the abnormalities found in blood tests (Calcium, phosphate, 25-hydroxy-vitamin D, 1,25-dihydroxy-vitamin D, Parathyroid hormone, alkaline phosphate):
Osteomalacia may be suspected on a clinical basis, especially when there is a family history or lab abnormalities listed on the table above. In uncertain cases, the most reliable way to establish the diagnosis is with an UNDECALCIFIED bone biopsy. Click images for larger views

| NORMAL: A photomicrograph of a biopsy from a normal postmenopausal woman showing an osteoid seam of normal width. Mineralized bone is green and osteoid is orange. | |

| 
| OSTEOMALACIA: The orange-staining osteoid covers many surfaces and is thicker than normal. The second photo is from part of the biopsy that was decalcified and thus it appears normal. The osteomalacia cannot be appreciated. |

| FOCAL OSTEOMALACIA: Both photos from the same section of a bone biopsy. Near the cortex is osteomalacia. This woman had been misdiagnosed as Paget's disease and had been treated with high doses of etidronate. | |

| ALUMINUM STAIN. This was from a dialysis patient with severe osteomalacia. Aluminum stains as a red line on the surface and in cement lines. | |

| 
| VITAMIN D DEFICIENCY. The second biopsy shows resolution of the osteomalacia after treatment. |
Click to view an animation of normal remodeling, then compare to osteomalacia. These are Flash animations. Use your browser's 'back' button to return.
Normal | 
Osteomalacia |
Click photos for enlarged view.
 Here is an xray showing a pseudofracture (red arrow) from an adult who has x-linked hypophosphatemic rickets. This is a classic pseudofracture and is pathognomonic for osteomalacia. |  This is an xray of a child with bowed legs due to rickets (thanks to Dr. Mike Richardson) |

Closer view of a knee showing thick growth plates that appear fuzzy, and widened knee joints |
This really depends on the cause of the osteomalacia. Treatment can be as simple as vitamin D or as complex as parenteral nutrition. Orthopaedic surgery is frequently necessary. Patients with X-linked hypophosphatemic rickets usually are treated with a combination of calcitriol and phosphate supplements, and careful medical monitoring is needed.
| Phosphate supplements | ||||
| Name | ID | Composition | Phosphorus mg/dose | |
| K-Phos MF (Beach) | White, 1135 round | KPO4 155 mg NaPO4 350 mg | 125 | 
|
| K-Phos #2 (Beach) | Brown, 1134 oblong | KPO4 305 mg NaPO4 700 mg | 250 | 
|
| K-Phos Neutral (Beach) | White, 1125 oblong | KPO4 155 mg Na2PO4 852 mg NaPO4 130 mg | 250 | 
|
| K-Phos (Beach) "Original" | White, 1111 round | KPO4 500 mg | 114 | 
|
| Neutra-Phos K (Alza) | powder | KPO4 and K2PO4 1450 mg | 250 | |
| Neutra-Phos (Alza) | powder | NaPO4 and K PO4 1250 mg | 250 | |
| Phospha-Soda (Fleet's) | solution | NaPO4 | 125 mg/mL | |
| (250mg phosphorus = 8 mmol). Adult dose varies, 1000 - 2000 mg/day | ||||
Burosumab is a new medicine that was approved in April 2018 for use in patients with X-linked hypophosphatemic rickets. This medicine is a monoclonal antibody against FGF-23. A paper by Carpenter reports the findings in a clinical trial of pediatric patients.
I intend to add more information about this new medicine as soon as possible.
X-linked Hypophosphatemia Network. This is an outside site about hereditary hypophosphatemia with rickets, usually x-linked (previously called vitaminD resistant rickets). It is written and maintained by a support group of patients who have XLH. And here is a good review article for clinicians: (Carpenter).
Hypophosphatasia has a totally different pathophysiology from the other kinds of osteomalaica. It is caused by deficiency in the enzyme alkaline phosphatase. There are several isoforms of this enzyme with different functions; the bone form cleaves pyrophosphate. This is important because the pyrophosphate acts to inhibit mineralization. Without it, we would all turn into pillars of calcium-phosphate! The bone must be protected from this inhibition, and so the bone is entirely lined with lining cells that contain alkaline phosphatase. When the enzyme doesn't work, the pyrophosphatase enters the bone and prevents mineralization. In homozygous cases the disease is fatal because the bones of the ribs are so weak the children get pneumonia and breathing difficulty. Diagnosis is suspected if alkaline phosphatase is low and confirmed with elevated levels of plasma pyridoxal 5'-phosphate and urine phosphoethanolamine.
When the symptoms appear later in childhood, the disease severity is variable. Some children will have rickets as well as dental problems, others may have only mild bone disease
In adults, partial deficiency of alkaline phosphatase causes osteomalacia, bone pain and stress fractures. Patients also suffer from arthritis and chondrocalcinosis, as well as dental abnormalities. Calcium and vitamin D should be given carefully, and NOT in high doses, because extra calcium will make the calcinosis worse. Teriparatide might be beneficial in adults with hypophosphatasia (Whyte MP).
 New!
New! This is a new medication which can treat the serious cases of hypophosphatasia. It replaces the alkaline phosphatase and is given by injection three times a week. This has been dramatically effective in children with the severe forms, who are now able to grow and begin normal activities. In adults it can heal the osteomalacia.
more about this new medicine soon!
The bisphosphonates are analogs of pyrophosphate; when a carbon is substituted for the oxygen the molecule can enter the bones and inhibit mineralization. This is why high doses of older bisphosphonates like etidronate cause osteomalacia. Newer bisphosphonates are more potent so the doses given are not high enough to cause osteomalacia.
Also related to pyrophosphate is a newly defined form of osteomalacia caused by a mutation in ENPP, which generated pyrophosphate(Lorenz-Depiereux B). Loss-of-function ENPP1 mutations cause both generalized arterial calcification of infancy and autosomal-recessive hypophosphatemic rickets. Am J Hum Genet 2010;86(2):267-72.
Vitamin D deficiency is the most common form of osteomalacia, and is usually due to a combination of low dietary vitamin D plus lack of exposure to sunlight. Examples are babies who are kept out of the sun and drink breast-milk, which does not contain much vitamin D. Elderly people in nursing homes who don't take vitamins are also at risk. Women who have moved to London from Arabia get this form of osteomalacia because their clothing prevents sun exposure and they don't drink dairy products .
Patients with intestinal disease, such as cystic fibrosis, celiac sprue and bypass surgery for obesity, are prone to vitamin D deficiency. Even if they take supplements, the vitamin D is not absorbed or is broken down too quickly.
More about Vitamin D
Oncogenic osteomalacia is a very rare disease. Recently there have been many studies of the hormones that are secreted by these tumors, because they help us to understand the physiology of bone. There is also a new report that some patients respond to cinacalcet.
More about oncogenic osteomalacia.
Dentin Matrix Protein 1 (DMP1) is made in the osteocytes. Homozygous mutations in this gene on the 4th chromosome cause osteomalacia. The DMP1 somehow inhibits secretion or production of FGF23, so the mutated protein releases the inhibition. Also, the osteocytes have abnormal morphology (Feng JQ and Lorenz-Depiereux B.)
Imatinib , a drug used to treat certain cancers (CML or gastrointestinal stromal tumors) causes hypophosphatemia, renal phosphate wasting, and biochemical evidence of low bone turnover. The mechanisms are not clear - - - the authors suggested it was due to suppression of the RANK-L signalling, but other drugs which block bone turnover, or which directly block RANK-L signalling do not cause low phosphate. (Berman E).
A Klotho mutation has been described, leading to osteomalacia (Brownstein CA). Read more about Klotho
Autosomal dominant rickets becomes worse with iron deficiency. The osteocytes in both normal people and those with a mutation in FGF23 will secrete more FGF23 when there is iron deficiency. However, in the normal people the FGF23 is degraded, whereas in those with the mutation the FGF23 levels increase and cause phosphate loss (Imel.)