
A study by Leslie WD of over 16,000 Canadian women, found that total hip BMD alone maximized overall osteoporotic fracture risk prediction. When there was a discrepancy between total hip and femoral neck, the total hip was more related to fracture risk. The spine measurement did not improve the fracture prediction. However, in this large study, only the clinical (symptomatic) spine fractures were included and the patients did not get routine xrays to see if they had actually developed a compression fracture of the spine. A subsequent study found that spine bone density predicted clinical vertebral fractures (hazard ratio 1.84 per standard deviation) and hip bone density predicted non-vertebral fractures (HR 1.66 per standard deviation). Using both measurements modestly improved overall fracture prediction if the discrepancy was more than one standard deviation. They then derived a modification of the FRAX prediction tool, which is described on the risk calculator page.
This image shows the prevalence of discordance in clinical centers, which generally show that about 5% of patients have major discrepancy between the hip and spine bone density, and another 30 to 40% have minor discrepancies.
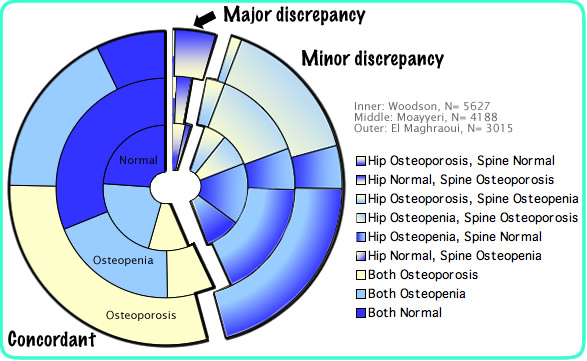
Here is a "collapsed" view of the same data plus the results from the Study of Osteoporotic Fractures, showing those who have osteoporosis (T-score less than -2.5) in the spine, the hip, both or neither. The osteopenia results were combined with the normal ones.

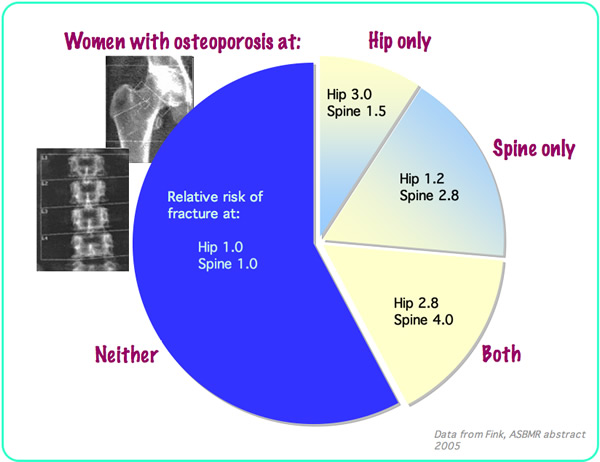
Just because there is a discrepancy does not mean that one measurement is better or more sensitive than another. What is necessary is to know how these data predict fractures! The SOF study (ASBMR abstract 2005) followed the women for 11 years and found that bone density predictions were site specific: For example, if bone density shows osteoporosis at the spine but not the hip, then the risk of a hip fracture is only 1.2 times the risk of somebody without osteoporosis, but the risk of a spine fracture is 2.8 times the risk of somebody without osteoporosis.
There are also many technical reasons for discordance, including artifacts outside the body (zippers, coins, knives, etc). Some reasons are physiological. Here are some examples:
| Spine higher BMD | Spine lower BMD | Hip higher BMD | Hip lower BMD |
|---|---|---|---|
|
*Arthritis *Ankylosing spondylitis *Aortic calcifications *Compression fractures *Chronic Kidney Disease *Calcium tablets *Navel jewelry |
*Estrogen deficiency *Glucocorticoids *Scoliosis (sometimes) *Laminectomy | *Exercises *Paget's disease *Blastic lesions | *Spinal cord injury *Hyperparathyroidism *Regional osteoporosis *Lytic lesions *Fibrous dysplasia |
Here is an Excel file that briefly reviews some of the papers about this.
Updated 5/2/08 