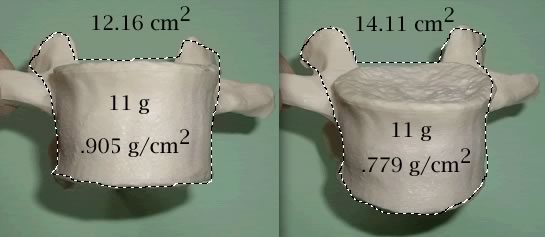
These issues may become important when interpreting the areal measurements used in DEXA. For example, observe the difference in the BMD from rotating a vertebra downwards:
Depending on the rotation, patients with scoliosis may appear to have higher or lower bone density than the actual value, if you could measure it in 3-dimensions. Some people with scoliosis also have arthritis and sclerotic changes in the vertebrae, which will increase the bone density. The bone responds to mechanical forces, and so the concave side (more compression) is denser than the convex side. Other people with scoliosis have diseases that limit activity or result in other secondary causes of osteoporosis. For these reasons, the spine bone density in a patient with scoliosis should not be used in fracture prediction.
Everybody has a different shape - - - this also applies to the vertebrae. Some people have short, squatty vertebrae, others are tall and narrow. This can be independent of size and can cause errors not corrected with BMAD.
Here are some references:
Routh RH. The relationship between bone mineral density and biomechanics in patients with osteoporosis and scoliosis. Osteoporos Int 2005;16(12):1857-63.
Rumancik S. Assessment of bone quantity and distribution in adult lumbar scoliosis: new dual-energy x-ray absorptiometry methodology and analysis. Spine 2005;30(4):434-9.
Cheng JC. The effect of vertebral rotation of the lumbar spine on dual energy X-ray absorptiometry measurements: observational study. Hong Kong Med J 2001;7(3):241-5.
Girardi FP. Correlation between vertebral body rotation and two-dimensional vertebral bone density measurement. Osteoporos Int 2001;12(9):738-40.
Pappou IP. Discordantly high spinal bone mineral density values in patients with adult lumbar scoliosis. Spine 2006;31(14):1614-20.
Updated 8/15/08

