{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
 MORPHOMETRY OF HUMAN LUNG
MORPHOMETRY OF HUMAN LUNG TOXICOLOGY OF THE LUNG (2)
ˇˇ
ˇˇ
I. Pulmonary Anatomy and Ultrastructure
The lung is organized into 3 compartments: airways, blood vessels, and conective tissue. We can think of it as 2 systems of tubes (airways and vasculature) cemented together by the third compartment (inteerstitium):
- Airways and airsacs (traqueobronquial tree and alveoli),
- Vasculature (2 systems, bronquial and pulmonary)
- Interstitium (systems: lymphatic, nervous; cellular: fibroblasts, muscle, nerve cells; extracellular: collagen, elastin)
The following slides review the overall gross anatomy and hystology of the lung and its cell types, examine some of its morphometric (quantitative) features, and show some structural features revealed by specialized morphological techniques.
A. Structural schema
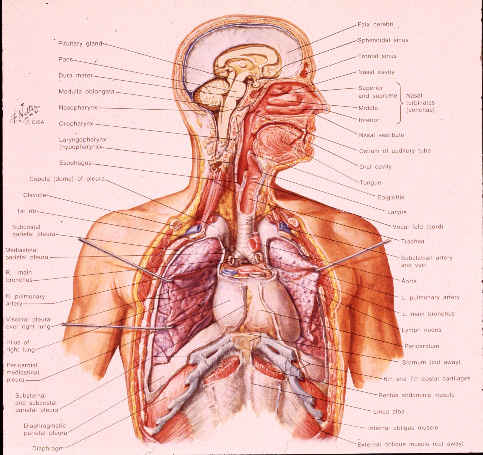
Slide 1. Netter, p. 3. Respiratory system. Note the distinction between the upper and lower respiratory systems. The function of the nasal passages: inhaled air is "conditioned", ie, warmed and humidified and it can also be the site of toxic action, e. g., formaldehyde.
Slide2. Netter, p. 16. Bronchopulmonary segments. Lobes of human lung: 3 right lobes with 10 segments and 2 left lobes with 9 segments. Major airways on right are straighter than those on left.
Slide3. Netter, p. 24. Intrapulmonary airways.
Slide4. Intrapulmonary blood circulation.
Slide 5. Drawing of 3 levels of respiratory epithelium - alveolus, bronchiole, bronchi- with continuous airway lining fluid. In: Bergofsky. '91 Am J Med 91: 4s-10s.
ˇˇ
B. Ultrastructure and morphometry
Slide6. Netter, p. 26. Ultrastructure of respiratory epithelium.
Slide7. E. M. of bronchiolar epithelium.
Slide8. SEM of airway surface of adult monkey.
Slide9. SEM of fetal monkey lung with bronchial displasia.
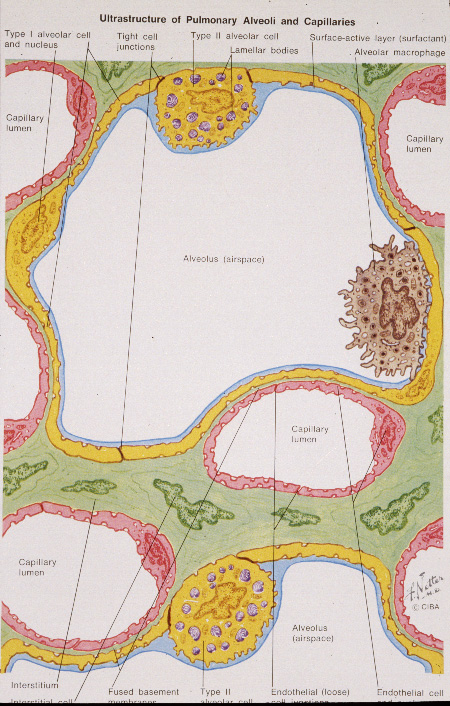
Slide 10. Netter, p. 29. Ultrastructure of alveolar capillary unit.
Slide 11. Netter, p. 30. Ultrastructure of the type II cell and surfactant secretion.
Slide 12. Drawing of mucocilliary blanket. In: Vander et al '70 Human Physiology. The arrows indicate the upward direction in which the cilia move the overriding layer of mucus, to which foreign particles are stuck.
Slide 13. Low mag SEM of mucous blanket in rat.
Slide 14. Higher mag SEM of mucous blanket.
Slide 15. TEM of mucous blanket.
ˇˇ
C. Specialized techniques
Slide 16. Airway cast-untrimmed.
Slide 17. Airway cast-trimmed.
Slide 18. Plastic cast of the conducting airways from traquea to terminal bronchioles, different color in each lobe.
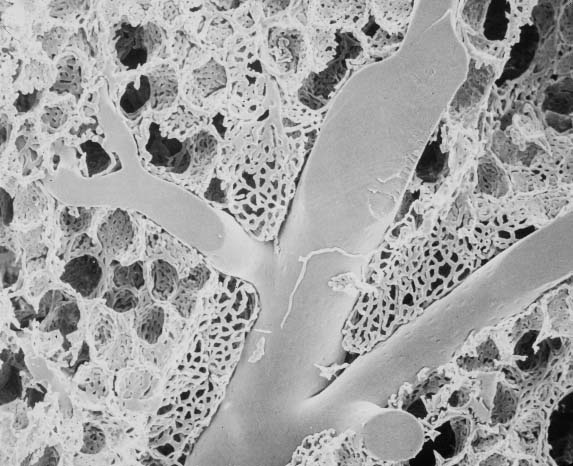
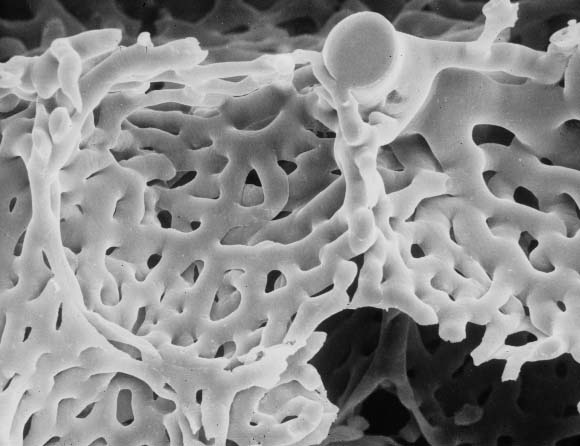
Slide 19. Low mag SEM of vascular cast.
Slide 20. Higher mag SEM of vascular cast.
ˇˇ
ˇˇ
ˇˇ
Cell Types in Normal Lung
More than 40 cell types have been identified (Breeze & Wheeldon, Am Rev Resp Dis,
'77).
| Airway epithelial cells | Connective tissue cells |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cartilage |
| Alveoli |
|
|
Muscle |
|
|
| Glands | Nervous |
|
|
|
|
| Vasculature | Pleura |
|
|
|
ˇˇ |
HISTOLOGICAL FEATURES OF LOWER RESPIRATORY SYSTEM
| Trachea & Bronchi: | Epithelium | ciliated cells |
| mucous-secreting cells | ||
| basal cells | ||
| Walls | cartilage (cells & ECM) | |
| smooth muscle | ||
| fibroblasts | ||
| collagen, elastin | ||
| Bronchioles: | Epithelium | ciliated cells |
| Clara cells | ||
| basal cells | ||
| ˇˇ | Walls | no cartilage |
| ˇˇ | collagen, elastin | |
| Alveoli: | Epithelium | type I cells |
| ˇˇ | type II cells | |
| ˇˇ | Walls | basement membrane |
| ˇˇ | collagen, elastin | |
| Terminal bronchiole | the last purely conducting airway | |
| Respiratory bronchioles, Alveolar ducts | are gas exchange airways; that is, have outpocketings of alveoli | |
| Bronchial vasculature | extends to terminal bronchioles | |
| Smooth muscle | extends to alveolar openings | |
| Lymphatics | start at alveolar/respiratory bronchiole junction | |
ˇˇ
MORPHOMETRY OF HUMAN LUNG
ˇˇ

| VL= | VA + | VNP + | VT + | VC + |
| 5 liters | 3800 ml + | 500 ml + | 450 ml + | 250 ml |
| ˇˇ | (76%) | (10%) | (9%) | (5%) |
| where: | VL | = total lung volume | ||
| ˇˇ | VA | = alveolar air space | ||
| ˇˇ | VNP | = major airways and blood vessels | ||
| ˇˇ | VT | = alveolar septal tissue | ||
| ˇˇ | VC | = alveolar capillaries | ||
(NP = "non-parenchyma"; versus
"parenchyma"the gas exchange portion of the lungmade up of alveoli, capillaries
and connective tissue)
Surface Area:

| Alveolar Number: | Estimated at 300 million in adult human. | |
| SA= | with LM | 60 m^2 to 80 m^2 |
| with EM | 160 m^2 | |
where: SA = alveolar surface area
ˇˇ
ˇˇ
TOXICOLOGY OF THE LUNG (2)
Summary of characteristics of human lung diseases
Inflammation: Acute or chronic response to cell/tissue injury; accompanied by influx
of inflammatory cells (macrophages, neutrophils, lymphocytes) and mediator release
(interleukins, cytokines).
Bronchitis/Bronchiolitis: Inflammation of airways; enlargement of mucous glands and
increased mucous cells; accompanied by airway narrowing by mucous plugs and air blockage,
edema, inflammation, and fibrosis.
Edema: Leakage of fluid from vascular compartment to interstitial and air
compartments.
Bronchial asthma: Heightened reactivity of bronchial tree to stimuli leading to
bronchial constriction and inflammation. Wheezing, cough, dyspnea, and tenacious sputum
may be present.
Emphysema: Destruction of and permanent loss of septal walls of alveoli, alveolar
ducts, and respiratory bronchioles.
Allergic alveolitis (hypersensitivity pneumonitis): Tissue reaction to inhaled
antigenic organic aerosols; leads to infiltration of lung by inflammatory cells and can
result in edema, fibrosis, and emphysema.
Fibrosis: Irreversible thickening of alveolar septa/airways by formation of
fibrotic (scar-like) tissue; may be associated with edema, presence of inflammatory cell
response.
Acute airway injury
 ctor cells, e.g., neutrophils
ctor cells, e.g., neutrophils
Acute lung (parenchymal) injury
General sequence of acute inflammatory response 
Chronic obstructive airway disease
Two major obstructive diseases:
1) Bronchi  al asthma
al asthma
2) Chronic obstructive pulmonary disease (COPD)
A) Chronic bronchitis (clinical state: pink puffers)
B) Emphysema (clinical state: blue bloaters)
ˇˇ
ˇˇ
Chronic lung disease (fibrosis)

| Fiber | Disease |
| asbestos | asbestosis (white lung) |
| silica | silicosis |
| cotton dust | byssinosis (brown lung) |
| aluminum dust | aluminosis |
| tin | stanosis |
| coal dust | pneumonconiosis (black lung) |


ˇˇ
The lung's defense against environmental pollutants
MAJOR PULMONARY OXIDANT SCAVENGERSa
| CATEGORY | ACTIONS |
| Catalase | Catalyzes dismutation of H2O2, reduces methyl and ethyl hydroperoxides. |
| Superoxide dismutases |
Catalyze dismutation of ·O2 to H2O2 |
| GSH redox cycle GSH peroxidase |
Catalyzes reduction of H2O2 and other hydroperoxides (lipid peroxides, lipoxygenase products). |
| GSH reductase | Catalyzes reduction of low-molecular weight disulfides. |
| G-6-PD and 6- phosphogluconate dehydrogenase |
Supply NADPH to the GSH redox cycle. |
| Vitamin E | Converts ·O2, ·OH, and lipid peroxyl radicals to
less reactive forms. Breaks lipid peroxidation chain reactions. |
| b-carotene | Scavenges ·O2, reacts directly with peroxyl radicals. |
| Bilirubin | Chain-breaking antioxidant. Reacts with ROO? |
| Vitamin C | Directly scavenges ·O2 and ·OH. Neutralizes oxidants from stimulated neutrophils. Contributes to regeneration of vitamin E. |
| Uric acid | Scavenges ·OH, ·O2, oxoheme oxidants, and peroxyl radicals. Prevents oxidation of vitamin C. Binds transition metals |
| Glucose | Scavenges ·OH |
| Cysteine | Reduces various organic compounds by donating electron from sulfhydryl groups. |
| Cysteamine | Same as cysteine |
| GSH | In addition to role as substrate in GSH redox cycle, reacts directly with ·O2, ·OH, and organic free radicals. |
| Taurine | Conjugates xenobiotics, reacts with HOCL. |
| Tracheobronchial mucus |
Scavenges inhaled oxidants. |
| Albumin | Binds transition metals. Reacts with oxidants as a "sacrificial" antioxidant. |
a In: Principles & Practice of Envir. Med. AB Tarcher, ed (1992), p. 113.
LINKS OF INTEREST
Link 1: Pulmonary pathology slides; some interesting ones about emphysema, mesothelioma, etc.
Link2.
ˇˇ