|
| The bisphosphonates increase bone mass in both cortical and trabecular bone. In this slide from the FIT study, the dose was doubled at year 2. |
|
| The biochemical markers of both bone resorption (N-telopeptide) and bone formation (Bone specific alkaline phosphatase) show dramatic decreases with the bisphosphonates. |
|
| The bisphosphonates cause dramatic reductions in the bone formation. This is seen on bone biopsies labelled with tetracycline. The graph shows the mineralizing surface as a percentage of the trabecular bone surface. With higher doses only 0.16% of the surface is still forming bone. |
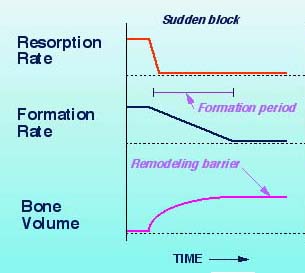 | EFFECTS OF BLOCKING RESORPTION Bisphosphonates block resorption, but formation continues for a forming period (6-12 months). During that interval the bone volume (and bone mass) will increase. This is a one-time increase, and afterwards the bone volume will plateau. The slight increases seen after a year probably represent increased mineralization within each newly formed bone remodeling unit. The mineral is more densely packed and so the bone density will increase even though the bone volume does not. |
|
NORMAL TURNOVER 650K | This animation shows a slice through a piece of bone about a millimeter long. It lasts 13 seconds and shows 30 months of "real time." The view is similar to the view seen under the microscope of a bone biopsy from a patient. The animation is derived from measurements of the bone surfaces and tetracyline labelling. There are about 10 BMU's in this view, each at a different stage. The bone formation rate in this movie is a bit above average, but within the normal range. |
|
ESTROGEN DEFICIENCY 660K | This animation starts the same place as the one showing normal turnover. The initial bone volume is 25%. The movie then shows what happens with estrogen deficiency. The resorption cavities are deeper and they occur more frequently. With these small changes, the individual BMU does not seem very different. But there are more BMU's and the trabeculae become perforated. They lose strength and have microfractures with microcallus formation. By 30 months the bone volume has decreased to 22%. Note that the width of the individual trabecula are normal. (Go to estrogen). |
|
BISPHOSPHONATE THERAPY 870K | This animation starts after the estrogen deficiency. The first 6 months show high turnover; then the little blue diamonds representing a bisphosphonate start to attach to the bone; resorption stops suddenly and formation stops after a few months. The bone continues to become more mineralized (darker), and only a few BMU's are still active. |
Etidronate may act by causing chemical changes to the mineral itself, inhibiting crystal formation and making the mineral resistant to resorption. These effects depend on the amount of drug given. With the newer bisphosphonates, the dose is so small that the effects cannot be caused by physical-chemical changes in the mineral.
Osteoclasts are the cells which mediate the effects of the bisphosphonates. There is evidence for both direct and indirect effects, which may depend on whether the cells are exposed to external drug or whether they ingest it along with the bone. The bisphosphonates also act on the osteoblasts, to either increase inhibitors or decrease promoters of osteoclast action or recruitment. There is no general consensus about which mechanism is predominant in vivo, and the mechanisms may be different for each bisphosphonate.
|
| These figures from a recent paper by Van Beek show the mevalonate pathway of cholesterol synthesis. HMG CoA reductase inhibitors such as mebastatin, used to treat hypercholesterolemia, had been shown to reduce bone resorption. Ibandronate inhibited bone resorption (shown as the lower dotted line). When geranylgeraniol was added, the inhibition was reversed. This was seen in the nitrogen-containing bisphosphonates (risedronate, alendronate, olpadronate, & ibandronate). GeranylgeranylPP modifies (prenylates) a small GTP-binding protein called rho21, which regulates the cytoskeleton. Thus, inhibition of geranlygeranylPP leads to abnormalies in the cytoskeleton, so osteoclasts don't have a ruffled border and are unable to resorb bone. |
| /__ |
|---|
| BACK to Bisphosphonates | FORWARD to Experimental therapy |
| __\ |
|---|
| Home page |
|---|