| BONE RESORPTION | |
| Abbr | Name |
| NTX | Aminoterminal cross-linking telopeptide of bone collagen |
|---|---|
| CTX | Carboxyterminal cross-linking telopeptide of bone collagen |
| PYD | Pyridinoline |
| DPD | Free Lysyl-pyridinoline (deoxypyridinoline) |
| TRACP | Tartrate-resistant acid phosphatase |
| Hyp | Hydroxy-proline (not very specific) |
| BONE FORMATION | |
| Abbr | Name |
| bone ALP, BAP | Bone-specific alkaline phosphatase |
|---|---|
| PINP | Procollagen type I N propeptide |
| OC | Osteocalcin (bone gla-protein) |
| ALP | Alkaline phosphatase (not specific) |
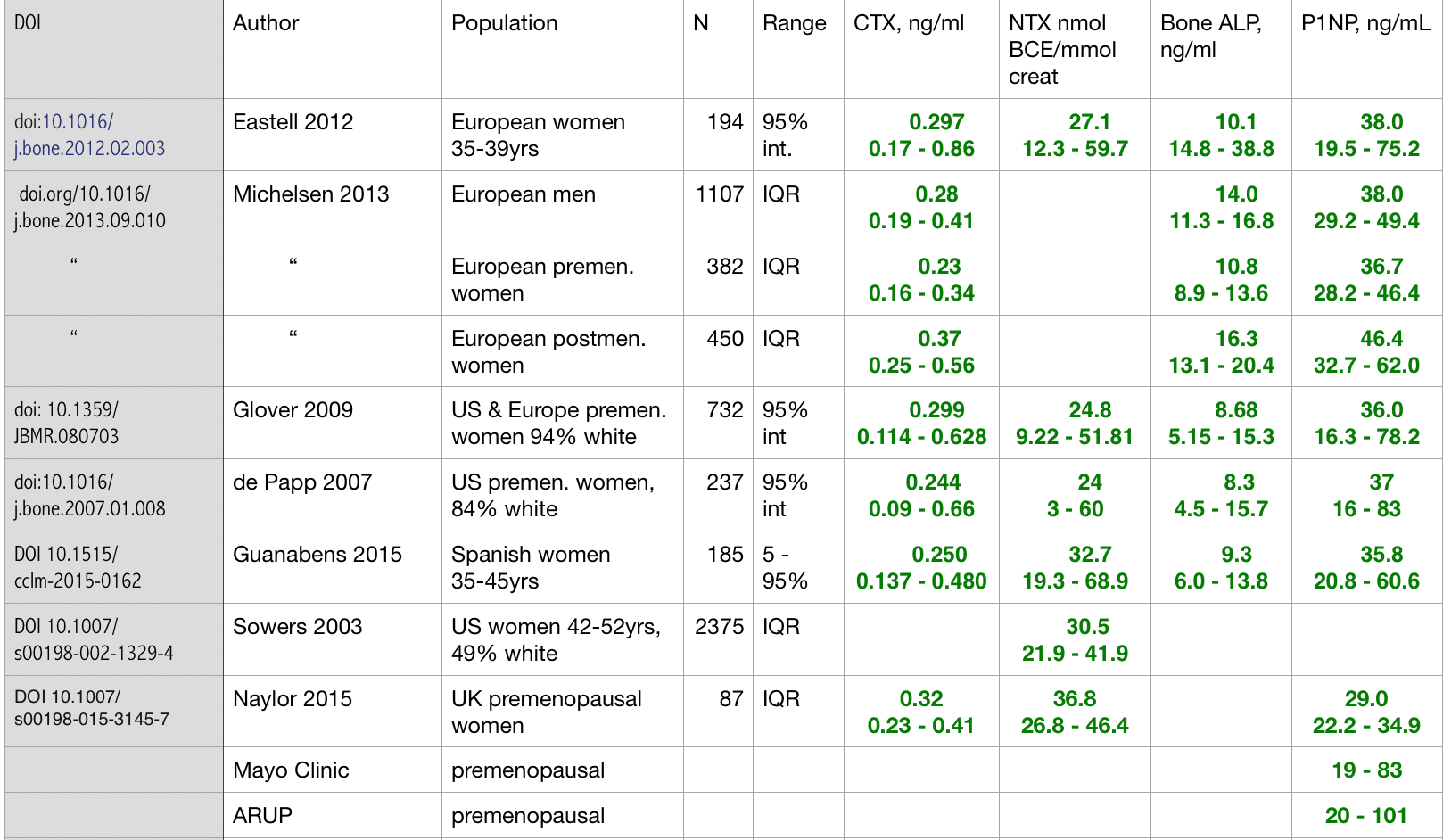
The biochemcal markers of bone formation and bone resorption are frequently called markers of "bone turnover." It is better to remember specifically which process is being measured, because sometimes the bone formation and resorption are not linked (for example, in early stages of steroid-induced osteoporosis, bone formation is low but bone resorption is high). These markers can NOT BE USED TO DIAGNOSE OSTEOPOROSIS! They help us understand the physiology of bone disease, especially in groups of patients or in clinical trials. For individual patients, the markers are not recommended for screening. Some recent studies advocate using them for monitoring osteoporosis treatment (Wu 2021), and they can be helpful in making treatment decisions.
In complicated cases these tests are indicated to provide information to the physician to help decide about future therapy. For example, if bone density decreases despite treatment with bisphosphonates, a high bone resorption would suggest either noncompliance or malabsorption of the medicine. If patients have discontinued denosumab, the resorption markers become very high and can be used to assess whether alternate treatment is working to prevent rebound bone loss. If bone resorption rate is low, it makes little sense to treat with anti-resorptive medications.
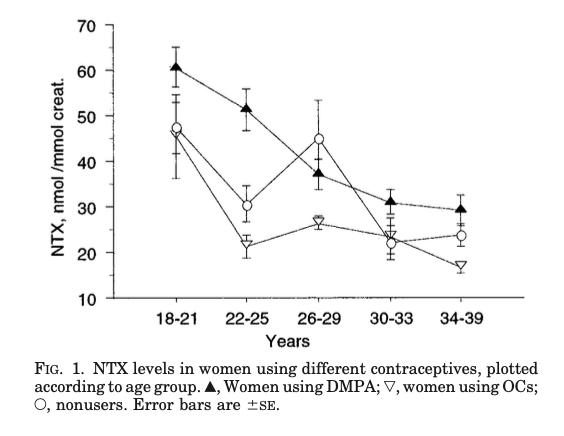
This graph shows NTX values in normal young women, according to contraceptive use. Note that the values decrease with aging, as the final growth plates fuse. From Ott.
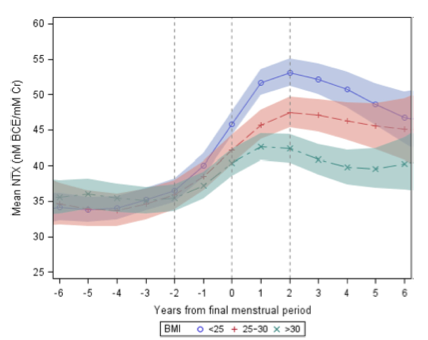
This graph, from a paper by Sowers, shows normal women from the Study of Women's Health Across the Nation, according to the time of their menopause. The blue color is from women who had the lowest body mass index, the red had BMI from 25-30, and the green were obese women. The colored shading is the 95% confidence interval around the mean value.
| What are they? | As shown in the animation above, they are cross-linking molecules which are released with bone resorption and excreted by the urine.(Knott, 1998) |
|---|---|
| Measure bone resorption | Calcium kinetic studies of bone formation and resorption show that the cross-links correlate highly with resorption. Also, these tests are higher in clinical situations previously known to have high bone resorption, such as Paget's disease and hyperthyroidism. (Eastell, 1997, Chavassieux, 2015, Weaver, 1997, Eriksen, 1993) |
| Very high levels in adolescents | Levels are high in children, who have a great deal of bone resorption associated with growth and modelling of the ends of the long bones. NTX levels reach a peak at about age 14, then gradually decreases to adult values. (Bollen, 1994, Mora, 1998, Szulc, 2000) |
| Increased after a fracture | In a prospective study, markers after a fracture were compared to those prior to the fracture. Markers were not altered in the immediate postfracture period but were clearly elevated during fracture repair, and remained elevated for up to a year after the fracture. (Ivaska, 2007) |
| Diurnal variation | Bone resorption is highest at night, and the values of NTX or CTX are highest in the early morning. The highest and lowest values are 24% different from the mean 24-hour value. (Bollen, 1995) |
| Correlations with BMD are modest | Correlation coefficients of NTX or CTX vs BMD in postmenopausal women vary from r = -0.3 to -0.5. These are statistically significant, but are not very useful for screening purposes. There are large errors in predicting the bone density for an individual person. (Marcus, 1999, Melton, 1997, Scariano, 2002) |
| Can't predict change in BMD | Most studies show that a value of NTX or CTX in a postmenopausal woman is not able to predict the change in BMD over the next one to three years, unless she is taking medication for osteoporosis. One would have expected that women with higher resorption rates would lose more bone, but the current techniques for measuring both resorption rate and bone density do not show such a relationship. Even if the techniques were perfect, they might not show a predictable relationship because the rates of bone formation also influence the change in the bone density. (Marcus, 1999) |
| Decrease with anti-resorptive therapy | Studies consistently show either NTX or CTX decrease about 40-80% with estrogen therapy or bisphosphonates. Furthermore, over 90% of patients who take the drugs have a decrease in the biochemical markers. (Ravn, 1999) |
| Cancer and other bone diseases | NTX or CTX tests help to assess the activity of other diseases such as Paget's disease (Vlot 2018) or metastatic bone lesions.(Chiu 2015, Ferreira 2016, Miyashita 2020) |
| Predict fractures | In a large prospective cohort of 7598 women older then 75, a high C-telopeptide level was associated with an increased risk of hip fracture with an odds ratio of 2.2. During the two years of study, 3% of those with a high C-telopeptide had a hip fracture. ( Garnero, 1996, Chopin, 2012). A study from Sweden found that high turnover markers were associated with fractures for up to 9 years in elderly women (Ivaska, 2010). |
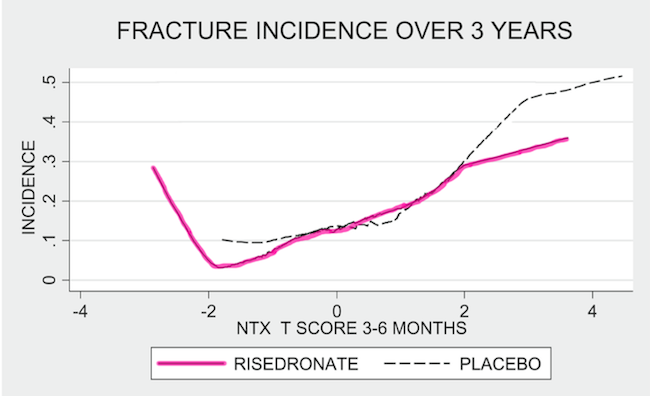
| Predict fractures with antiresorptive therapy | This graph shows the relationship between the urine NTX at 3-6months and the rate of fractures in the risedronate clinical trial. The pink line is the treated group and dashed line is placebo. In general, the lower the NTX, the lower the fracture risk, expect when the NTX was very suppressed there was an increase in fracture risk (Eastell, 2007) |
| What are they? | Osteoblastic activity is associated with serum osteocalcin, one of the proteins found in relatively high concentration in bone. Bone specific alkaline phosphatase (measured by radioimmunoassay, not by iso-enzyme analysis of alkaline phosphatase) is more sensitive and specific than alkaline phosphatase, this enzyme is made only by active osteoblasts. The the amino-propeptide of type I collagen (PINP) is currently the best marker of bone formation. Like many other proteins, collagen is secreted as a propeptide, and the ends are removed to synthesize collagen. |
|---|---|
| Measure bone formation | These tests have been shown to correlate with bone formation as measured by bone histomorphometry or calcium kinetic studies in normal individuals. Osteocalcin appears to be more closely related to formation of osteoid than to formation of mineralized bone. Thus, in osteomalacia or disease where there is excess osteoid such as Paget's disease, the osteocalcin may be inaccurate. Osteocalcin is excreted by the kidneys, and serum values are increased in renal failure. This may occur in elderly patients with normal creatinine who have low glomerular filtration rates. Assays which measure the intact protein are less influenced by the glomerular filtration rate. Bone specific alkaline phosphatase is not influenced by renal failure (it is frequently elevated, but that is because the bone formation rate is actually high). (Weaver, 1997, Chavassieux, 2015) |
| Relationship to resorption | In normal individuals the markers of bone formation follow the same pattern as the markers of bone resorption, because the two processes are coupled during bone remodeling. The levels are high during childhood and adolescence, low during adult years, and increase after menopause. They decrease following treatment with hormone replacement therapy or anti-resorptive drugs, but there is a lag between the decrease in the bone resorption markers and the bone formation markers. |
| Response to anti-resorptive therapy | In the alendronate Fracture Intervention Trial, (Bauer, 2004) each standard deviation reduction in the change of bone ALP was associated with fewer spine and non-spine fractures. The effect was at least as strong as that observed with a change in the BMD after a year. |
| Response to other therapy | Osteocalcin usually increases after treatment with 1,25-vitamin D. This may not represent increased bone formation, however, because histomorphometric studies of bone biopsies from women with osteoporosis treated with calcitriol have not shown any increase in tetracycline labelling. Fluoride causes increases in bone formation and in osteocalcin or bone alkaline phosphatase. PTH results in marked increases in these markers. |
| Increase with anabolic drugs | The role of these markers in diagnosis or treatment of osteoporosis is still uncertain. In complex or high-risk cases they may help to define the bone physiology. But they do increase with therapy with teriparatide, abaloparatide, or romosozumab. |

