
Pleural Effusions
Case 6 Answers
(This case is courtesy of Leo Bennett, MD, Madigan Army Medical Center.)
A 37 year-old woman presents with 10-days of progressive exertional dyspnea. Her review of systems was pretty unremarkable. She denied any fevers, chills, cough, sputum production or weight loss. The only recent event that she can recall was that she had an upper respiratory tract infection 3 months ago at the same time that multiple family members were sick. Her symptoms resolved without antibiotic therapy. Her only past medical history is allergic rhinitis. She is a life-long non-smoker and had a recent negative mammogram. A chest x-ray is performed and is shown below:
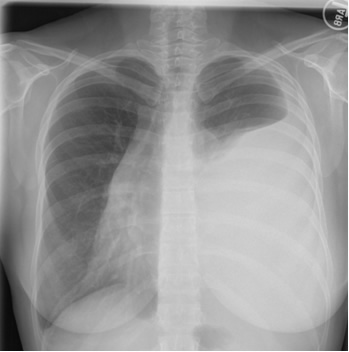
How would you interpret her chest x-ray?
This patient has what appears to be a large left-sided pleural effusion. It is also noteworthy that the trachea and mediastinal structures are shifted over to the right side of the chest. This could be due large fluid collection on the left but there might also be a large mass in the mediastinum and what appears to be the heart on the right side of the chest may actually be the shadow created by the mass.
Thoracentesis is performed revealing straw-colored fluid with 2875 RBC, 448 WBC (differential 18% polymorphonuclear cells, 37% lymphocytes, 35% macrophages and 10% mesothelial cells). The gram’s stain is negative. LDH 406 (serum value 180), total protein 4.7 (serum value 7.0). Cytology is performed and no malignant cells are seen.
How would you interpret the results of these pleural fluid studies?
The LDH is greater than the upper limit of normal for serum and the pleural fluid: serum ratio for LDH is > 0.6 while the pleural fluid: serum ratio for protein is > 0.5. This effusion, therefore, should be classified as an exudative process. The lymphocyte count of 35% is not high enough to be classified as a lymphocyte rich pleural effusion. However, in some cases macrophages can be confused on cell counting with lymphocytes and the true lymphocyte count might actually be a bit higher. The cytology is negative, but as noted earlier, this does not rule out the possibility of malignancy.
A CT scan of the chest is performed. Two representative images are shown below.
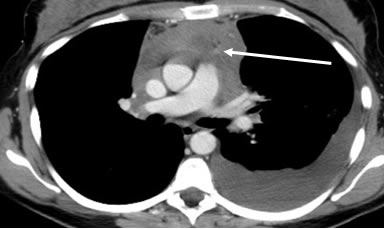
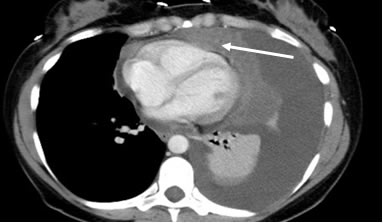
What are the noteworthy findings on the CT scan? What is the differential diagnosis for these findings?
The arrows in the CT scan images point to a large anterior mediastinal mass, the differential diagnosis of which includes: teratoma, thymoma, thyroid carcinoma and (terrible) lymphoma (the 4 T’s).
What further diagnostic steps are warranted?
Given the items on the differential diagnosis, this patient requires a tissue biopsy. This can be obtained by through a Chamberlain procedure in which a small incision is made in the anterior wall with dissection down into the anterior mediastinum or through a video-assisted thoracoscopic surgery. The patient in this case went on to have a surgical biopsy and was found to have lymphoma as the cause of her effusion.
UW School of Medicine : School of Medicine Mission
Copyright and Disclaimer : Credits and Acknowledgements