Risk factors for fractures
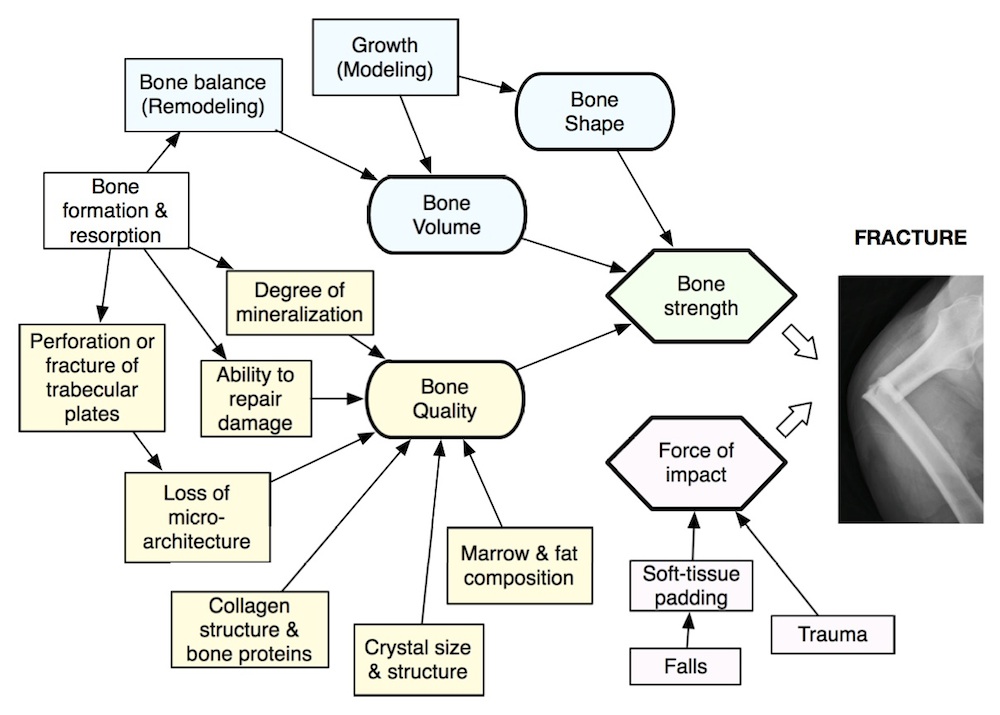
Fractures are a result of both trauma and decreased bone strength. Trauma depends on factors related to falling and to the force of the impact. For example, bones will break more easily when subjected to torque than compression. Bone strength depends on bone volume, shape and quality. The bone density is determined by the porosity (related to volume) and the degree of mineralization.
Bone density is an important risk factor
Bone mineral density (BMD) is usually measured using xrays.
 Many studies demonstrate the ability of bone density to predict fractures, especially fragility fractures (those caused by minor trauma). The lower the bone density, the greater the risk for a fracture. However, other factors must be taken into account. The risks depend also on which bone fractures, which bone is measured, the ethnicity, size, gender, and health of the person. There are more details about BMD and fracture risk in the section about bone density.
Many studies demonstrate the ability of bone density to predict fractures, especially fragility fractures (those caused by minor trauma). The lower the bone density, the greater the risk for a fracture. However, other factors must be taken into account. The risks depend also on which bone fractures, which bone is measured, the ethnicity, size, gender, and health of the person. There are more details about BMD and fracture risk in the section about bone density.

You can use the World Health Organization Fracture risk calculator to estimate the hip fracture risk based on the bone density as well as some other factors.
Epidemiological risk factors
AGE, GENDER, and RACE are important risk factors for osteoporotic fractures. Men and women who have the same bone density have about the same risk of a fracture, but overall women have more fractures because they have lower bone density. Persons of African ancestry have better bone density than other races; furthermore, at the same bone density they have about 30% fewer fractures (Cauley). Asians have fewer fractures than Caucasians even though their bone density is lower.
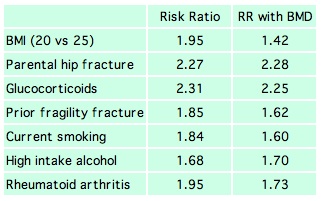 This chart shows the risk ratio for several important factors that are included in a WHO model of fracture risk prediction (Kanis) based on 9 cohorts including 46,000 men and women. These factors are chosen because they are significantly associated with fractures, are easy to assess, and are common enough to be important on a world-wide epidemiological basis.
This chart shows the risk ratio for several important factors that are included in a WHO model of fracture risk prediction (Kanis) based on 9 cohorts including 46,000 men and women. These factors are chosen because they are significantly associated with fractures, are easy to assess, and are common enough to be important on a world-wide epidemiological basis.  The risk ratios with BMD show the risks that are independent of bone density. For example, in addition to worsening the bone density, these factors can cause more falls or affect the quality of the bone. See the information on the pages about smoking, steroids, nutrition, and more details about other epidemiological risk factors.
The risk ratios with BMD show the risks that are independent of bone density. For example, in addition to worsening the bone density, these factors can cause more falls or affect the quality of the bone. See the information on the pages about smoking, steroids, nutrition, and more details about other epidemiological risk factors.
Fractures predict fractures
The presence of a vertebral fracture increases the risk of a new fracture
by about 4 times, even when adjusting for bone density!
| This shows the risk of vertebral fractures (%/year) in 3000 placebo-treated women in the FIT study, according to BMD of the hip, age and presence of baseline vertebral fractures.
Note how much higher the fracture rate is for women who had a prevalent fracture than for those without one.
You can read more details about vertebral fractures.
|
Falling and the force of impact
A fall to the side increases the risk of hip fracture
by about 6 times, compared to falls in other directions.
Greenspan showed that women who fell on their side had a relative risk of hip fracture of 5.7 compared to those who fell in other directions. This is a much greater risk than a lower bone density, in which a standard deviation decrease increased the risk by a factor of 2. Gait speed plays a role. Women who walk faster are more likely to have forward momentum, and if they fall they land on their wrist. This may lead to a distal radius fracture, but that is much less devastating than a hip fracture.
Other factors for falling and ways to prevent them are in the fall prevention page. This page also has data about hip padding.
Bone quality
Bone quality is determined by bone mass (as measured by bone density) and also by the
micro-architecture of bone, the crystal size and shape, the brittleness, the connectivity
of the trabecular network, the vitality of the bone cells, ability to repair micro-cracks, and the structure of the bone proteins. The fat cells, vasculature, neuronal pathways and bone marrow cells probably also influence the quality of the bone as well as the quantity of bone.
Read more details about bone quality.
Updated 2/10/2016

